
52M from Iran, immigrated to Canada 2013.
- He was born in Isfahan, the 2nd largest city in Iran.
- He spent 2 years in Turkey 2011- 2013, before moving to Canada.
- He worked as a truck driver, now on medical disability due to anxiety/depression
In 2013, in Canada, he presented to hospital with atypical chest pain. Chest x-ray and CT chest showed a pulmonary cystic lesion next to the right heart border.

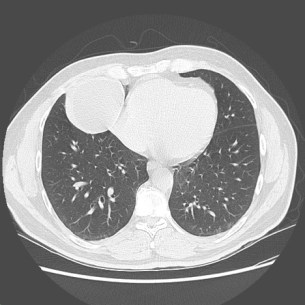
His cardiac CT confirmed a cyst next to the heart, no evidence of coronary artery disease. He was diagnosed with a probable benign pericardial cyst. The patient was followed by the internal medicine clinic until 2014, but no formal radiological follow-up was arranged

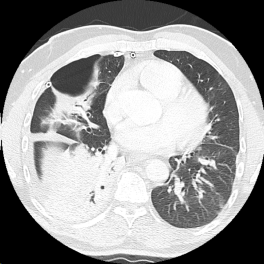
Five years later, in 2018 presented to hospital with sudden onset right-sided chest pain and shortness of breath. A chest x-ray revealed a right-sided pneumothorax, with some mediastinal shift to the left.

A chest tube was inserted in the emergency department. A CT scan the next day showed a tiny right-sided hydro-pneumothorax and a large cavitary lesion next to the heart.
 .
. 
Pleural fluid showed numerous hooklets and scoleces, which were diagnostic for hydatid cysts which had ruptured into the pleural space.
Images of the scolices….
He was diagnosed with a pulmonary echinococcal cyst that had ruptured into the pleural space and managed with albendazole 400 mg BID and pipericillin-tazobactam. There was no air leak noted. The pigtail pleural catheter was removed 1 week later.
However, a follow-up CT scan 3 days later showed interval development of a large loculated right pleural effusion, and worsening right middle lobe/right lower lobe opacity.

A chest drain was re-inserted. However, despite negative cultures from the drain, and ongoing broad spectrum antibiotics, his clinical deterioration deteriorated. He developed increased fevers, malaise and leukocytosis. As a result he was taken to the operating room and underwent right thoracotomy, right upper lobe and right middle lobe wedge resection. The procedure went well – operative note pending – and he was extubated in the intensive care unit the same day post-operatively.
Operative findings….
The operative cultures were negative and his broad spectrum antibiotics were discontinued on post-operative day x and chest tube removed on post-operative day x.
He was discharge home 11 days, on albendazole 400mg twice daily, with plans to complete 6 months of albendazole therapy to sterilize the spilled scolices.
Discussion
Comparison of echincoccal disease in Canada vs Eurasia.
Canadian strains seem to be much more benign in comparison with Euroasian strains!
Pulmonary echinococcus more common in children.
