
December 2018, a 67-year-old woman presented to the Emergency Department at VGH with an episode of pain in her left foot.
She had an over 20 year history of trouble with her left foot.
She described chronic, progressive swelling, deformity, disability and recurrent small wounds that burst and leak blood/pus.
She was from a small village in Gujarat India, and immigrated to Canada in 1996.
Timeline:
- 1990 (around then) – developed wounds and swelling on her left foot
- 1995 – still in India – foot slowly worse – surgery on the foot, took a long time to heal
- 1996 – moved to Canada
- 1999 – saw dermatology
- biopsy “tiny sulfur granule c/w actinomycosis” – but cultures negative
- treated with septra x 6 months, and may have have been some improvement
- 2008 – saw ID as still bothering her
- another biopsy – “nonspecific inflammation” – no organisms seem, cultures again negative
- restarted septra, but had GI upset, so switched to amox/clav – indefinite duration
- 2015 – still having recurrent sinus tracts and drainage
- another biopsy ”granulation tissue”- no organisms seen, cultures again negative
- continue amox/clav…
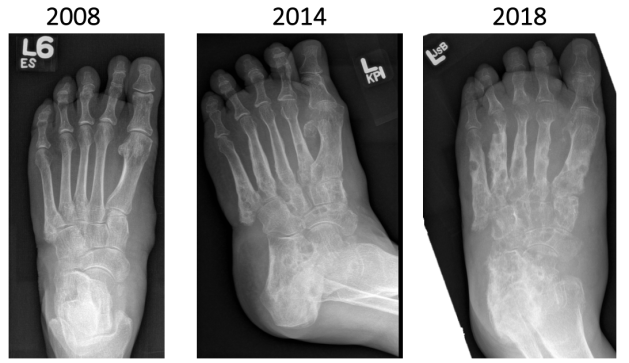
Appearance of foot December 2018…

X-rays…
CT scans…


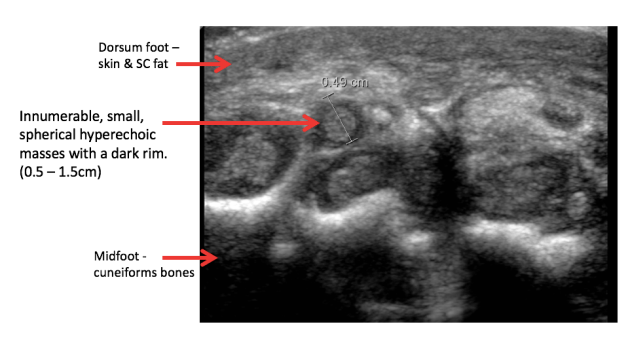
Underwent ultrasound guided biopsy of tissue from the midfoot….
Pathology…
a) Hematoxylin-eosin staining: Sulfur granules seen. Dense acute and chronic lymphoplasmacytic inflammation with clusters of filamentous organisms
b) Gram stain: Gram positive filamentous organisms seen. (Colour of gram stain appears very atypical due to fixative).
a) H&E stain b) Gram stain

Cultures from this biopsy are negative to date (at 2 weeks of incubation in media for bacterial fungal and mycobacterial growth)
She has been started on a combination of Meropenem IV (via home IV program) plus oral Moxifloxacin. Tentative plan is for at least 6 weeks of this IV regimen, and then step down to oral medications for 1-2 years.
We do not have cultures or drug susceptibility testing available to guide therapy. Possible choices would be rifampin plus moxifloxacin, septra or doxycyline.
Any suggestions?
