
Today the results of the long-awaited BENEFIT trial were presented at the European Society of Cardiology Meeting and simultaneously published online on the New England Journal of Medicine website. (BENEFIT stands for:BENznidazole Evaluation For Interrupting Trypanosomiasis Trial)
Chagas disease is caused by the Trypanosoma cruzi parasite which is transmitted to humans by triatomine insects. It is curable when treated early (with a 60-day treatment course of benznidazole). However, it is often not recognized at the early stages and, untreated, approximately 30% – 40% of chronic infections lead to cardiomyopathy within 10-30 years.
 (CDC)
(CDC)
Approximately 6 to 7 million people world wide are infected by T. cruzi. However, less than 1% of persons with T. cruzi infection have received treatment, despite current recommendations for early treatment. Untreated many have progressed to cardiomyopathy.
Whether antiparasitic treatment with benznidazole has any effect on the clinical course of disease for patients with already established heart disease is unknown.
The authors conducted a prospective, randomized study involving 2854 patients with established Chagas’ cardiomyopathy. Patients in 5 countries in South and Central America were randomized to receive benznidazole or placebo for 40 – 80 days and were followed for a mean of 5.4 years.
All patients had serologic evidence of Trypanosoma cruzi infection (the parasite that causes Chagas), as well as EKG changes and other cardiac abnormalities characteristic of Chagas cardiomyopathy.
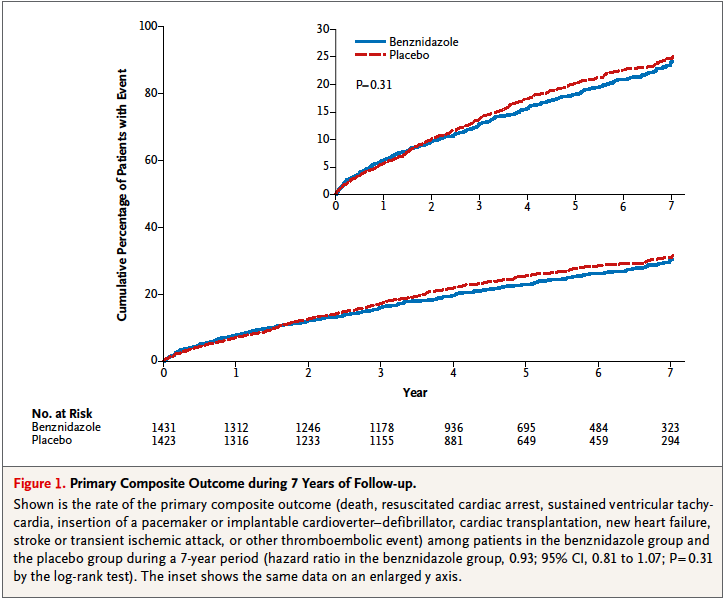
The primary outcome was a composite outcome of death, resuscitated cardiac arrest, sustained ventricular tachycardia, insertion of a pacemaker or implantable cardioverter–defibrillator, cardiac transplantation new heart failure, stroke, or other thromboembolic event.
Most patients (74%) had NYHA class I heart failure, and the mean ejection fraction (EF) was 55%. 23% had NYHA class 2 heart failure and 17% had an EF < 40%. The mean age was 55 years.
At baseline, a polymerase-chain-reaction (PCR) assay was performed on blood samples obtained from 1896 patients; 60.5% had positive results for Trypanosoma cruzi on PCR.
The trial showed that benznidazole had significant antiparasitic activity. The rate of conversion to negative PCR results were higher in the benznidazole group at the end of treatment (66.2% vs 33.5%), an effect that was not fully maintained after 5 years (46.7% vs 33.1%, both P<0.0001).
However, the rates of PCR conversion did not correspond to effects on clinical outcome and there was no effect on the primary clinical outcome. Tihe primary outcome occurred in 394 patients (27.5%) in the benznidazole group and in 414 (29.1%) in the placebo group (hazard ratio, 0.93; 95% confidence interval [CI], 0.81 to 1.07; P = 0.31).
 (NEJM)
(NEJM)
This trial is disappointing with respect to treatment options for those with heart failure.
Although the standard treatment with benznidazole may not be clinically effective in patients with established cardiomyopathy, treatment in the indeterminate phase (serology positive but no evidence of heart disease) may still be a window of opportunity and the role of early treatment needs to be further evaluated and improved.
As the authors of a related editorial point out, there is an urgent need for new drugs and new strategies for treatment – “The infected population with Chagas disease is aging, and time for them is running out.”
