
We discussed cholera in our weekly Tropical Medicine rounds today. Slides are posted in the UBC Tropical Medicine Rounds section.
Cholera is an acute diarrheal disease. Although most people affected have mild illness, about 2% can get extremely sick – cholera gravis – with over 10L diarrhea within 12 hours – leading to a rapid death.

Cholera is a disease of poverty and inequity. It is entirely preventable – and treatable with PO/IV fluids. Nobody should be dying of this infection in today’s world.
It is linked to inadequate access to clean water and sanitation.
There remains a tremendous global burden:
- 3 million cases per year (1.3 – 4 million)
- 100,000 deaths per year (21,000 – 143,000)
Yemen is currently the country with the world’s largest humanitarian crisis with more than 24 million people –80 per cent of the population – in need of humanitarian assistance.
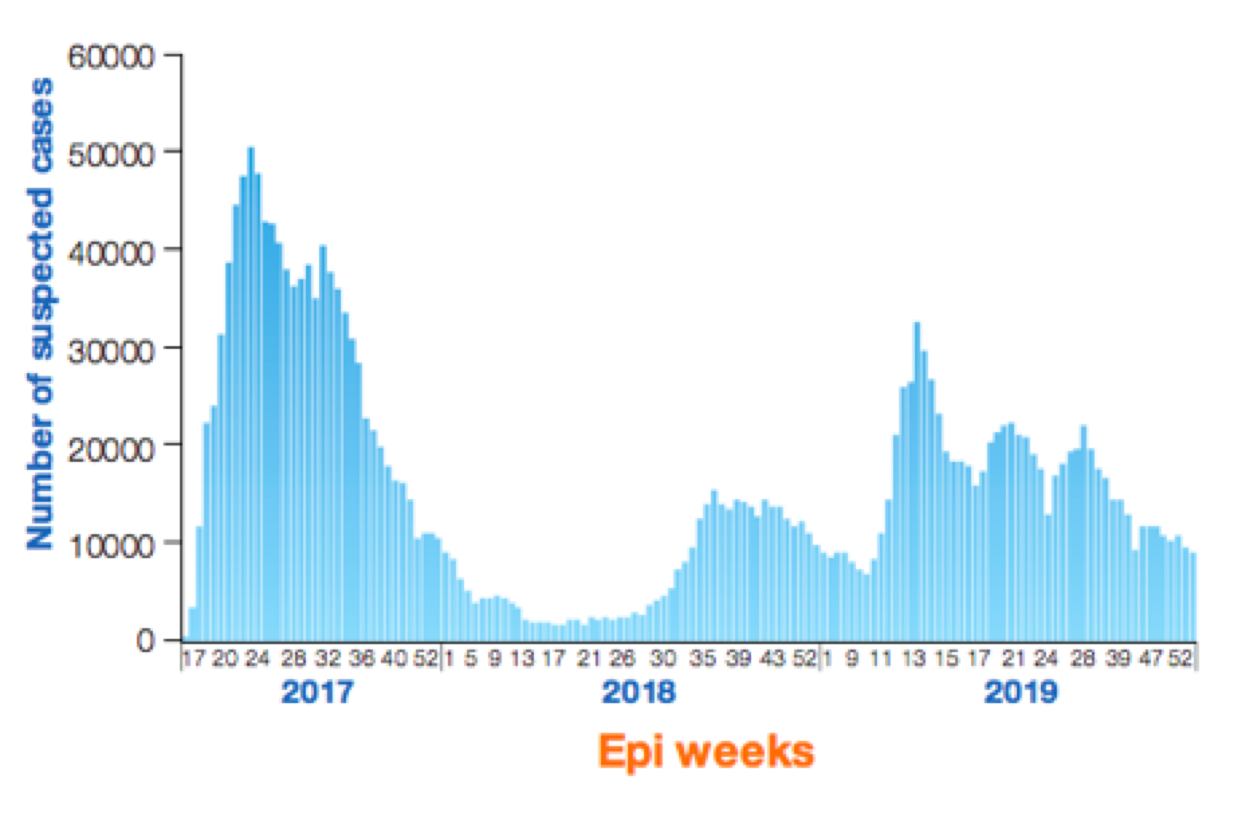
Yemen is also home to the largest epidemic of cholera in modern history with an estimated 1 million cases d 3,000 deaths since the civil war started, sewage systems failed, and the epidemic began in 2017.
There are safe, inexpensive, and effective Oral Cholera Vaccines now available. However, there has been limited uptake of these vaccines in key humanitarian emergencies and cholera epidemics.
The lack of OCV in the management of the cholera outbreak in 2010 after the devastating earthquake in Haiti received some media attention. A global stockpile was created, and has since been part of the national response to the epidemic in Haiti – as of today October 2020, no cases have been documented in the country for one year.
The use of OCV in the massive refugee settlements in Bangladesh created to assist the thousands of desperate Rohingya refugees fleeing for their lives from Myanmar has likely played a large role in staving off local epidemics of cholera.
In light of this, it is important to consider and question the delayed introduction of OCV as part of the humanitarian response to cholera epidemic in Yemen – the worst in modern history.
There was an excellent article on cholera in the NY times in 2016 – attached. The article concludes that “The world finally has a vaccine that, with routine administration, could end one of history’s great scourges.” And, as an explanation for the lack of widespread use of this lifesaving and cost-effective vaccine, a statement by Dr. Clemens, co-inventor of oral cholera vaccine, that “We’re probably not bad scientists, but we were lousy advocates.”
The challenges in Yemen are immense. There is a civil war going on. But, as COVID-19 has taught us, as clinicians responsible for people’s health and wellbeing, we also need to consider and address the inequities underlying illness – and question why some people are denied access to vaccines as effective as the oral cholera.
